|
||
|
TWN
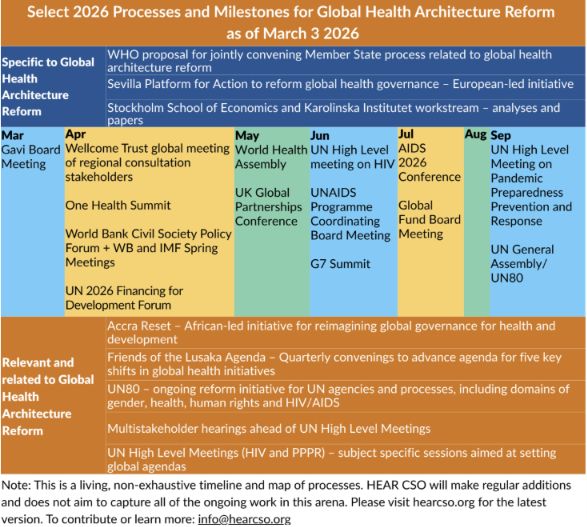
Info Service on Health Issues (Jul26/02) WHO: Reforming Global Health Architecture on Whose Terms? Kuala Lumpur, 10 July (Dian Maria Blandina*) – The global health architecture with its systemic flaws is poised for reform but on whose terms? Adopted at the 79th World Health Assembly (WHA79) in May 2026, the WHO Director-General’s proposal for a “Joint Process to Support Reforms of the Global Health Architecture and the UN80 Initiative” (Document A79/24) marks the most formal attempt in decades to address systemic failures in global health governance (GHG) that has disadvantaged the Global South. Document A79/24 cites the following reasons for the failure of the current global health architecture: fragmentation, donor dependency, weak country ownership, and entrenched governance asymmetries. While these are well documented, they are usually politically produced. It is a fact that the current GHG architecture is the result of shifting power from the United Nations bodies into a dense ecosystem of parallel fora, many of them shaped by US-EU preferences through the G7, Bretton Woods Institutions, and global public-private partnerships. The reform process establishes a Joint Task Force bringing together Member States, global health initiatives, UN entities, and the World Bank, which is intended to produce recommendations by WHA80 in May 2027. Thus, the institutional design of the process already mirrors the fragmented governance landscape it seeks to coordinate, i.e. actors that sit at the core of donor-influenced health financing architectures are now formal co-architects of a reform meant to discipline the very fragmentation they helped consolidate. The objectives of the Joint Task Force are: “i) enhancing the alignment of the mandates and capacities of GHA actors with the essential GHA functions and across global, regional and national levels; (ii) enhancing coordination and decision-making to strengthen collaboration, accountability and coherence across global, regional and country levels; (iii) aligning financing with national, regional and global priorities to advance national self-reliance and ensure sustainable and predictable support for global public health goods and regional functions.” The scope of the GHA includes essential” global health functions: setting norms, technical guidance and standards; data, monitoring and knowledge; surveillance and health security; product innovation and access; development cooperation for health (including the strengthening of national health systems to advance resilience and universal health coverage); and humanitarian emergency response. The process excludes the following aspects form the scope of the work will propose neither revisions to organizational mandates nor specific mergers or consolidations, which fall within the authority of the relevant governing bodies, and will not address disease- or intervention-specific approaches.” The joint process is to produce a preliminary report for the consideration of the WHO Executive Board and governing bodies of partner organizations, and the final report containing a road map for the implementation to be submitted to WHA80. Thus, the global health architecture (GHA) reform discourse focuses on architectural tweaks, i.e. reshuffling institutions and funding streams, as if the problem were technical rather than political, without acknowledging the decisions have led to the current situation. Fragmentation as a political project One of the important shortcomings of current GHA is the fragmentation and power imbalances. According to the abovementioned WHA document, “The substantial expansion in the number of health actors who were instrumental in achieving these gains has also added complexity and resulted in power imbalances, fragmentation and duplication, which are limiting country ownership, impact and equity.” Since the early 2000s, GHG witnessed the emergence of an archipelago of vertical initiatives, special funds, public-private partnerships, and issue-specific summits operating alongside, rather than within, the core constitutional machinery of the WHO and the wider UN system. These arrangements are often defended in the language of efficiency, agility, and innovation, but they also perform a clear political function: they allow major donors, especially the US and European powers acting through the G7, Bretton Woods Institutions, and philanthropic alliances, to shape priorities and financing modalities in spaces where they exercise greater leverage than in universal one-country-one-voice institutions. Formally, these mechanisms are open and collaborative. Structurally, however, influence is mediated by financial contribution, technical capacity, and institutional proximity to major Northern governments, banks, and foundations. The decision-making is therefore frequently decoupled from the premises of multilateralism, i.e. one member one vote and vested in a small set of actors. In order to seek legitimacy of limited participation of members in the governance, a multistakeholder governance model was mainstreamed. Thus, the GHG fragmentation reflected in the current architecture is not merely a proliferation of actors but a political strategy to disperse the authority across multiple entities including partially overlapping venues, in ways that dilute the bargaining power of the Global South while preserving the optics of inclusion. Despite widespread acknowledgment of its detrimental effects, fragmentation in GHG persists due to deeply entrenched, interconnected factors including the proliferation of actors, divergent interests, and power imbalances. An ongoing study is critically unpacking this fragmented architecture to identify structural opportunities for amplifying the voice and participation of the Global South. While the WHO is formally tasked with restoring coherence to a fragmented GHG, the joint reform process instead embodies the contradictory interests of its actors; crucially, most entities within the Joint Task Force on GHA reform are themselves products of that very fragmentation strategy. A reform proposal with built-in ceilings The proposal aims to foster a country-led, coherent, and inclusive global health ecosystem, but it also imposes clear limits on how far reform can go. In particular, the scope of GHA reform explicitly rules out recommending institutional mergers, mandate revisions, or disease-specific restructuring, thereby placing major elements of the fragmented health landscape beyond the reach of structural redesign. In effect, the reform process is tasked with improving coordination among institutions whose mandates, funding models, and political insulation are treated as largely fixed. This ceiling is not technical; it is political. It reflects a compromise with actors whose cooperation the process needs, but whose influence is bound up with the current institutional dispersion. The result is a reform architecture that can rationalize the system at the margins while avoiding the deeper question of whether the present distribution of authority across WHO, the World Bank, global health initiatives, and philanthropic actors is itself part of the problem. Representation choices reinforce this constraint. Regional health bodies are structurally underrepresented despite the rapid growth of regional health cooperation in response to supply disruptions, geopolitical tensions, and declining confidence in traditional donor channels. Civil society and affected communities, though often invoked in the principles of inclusiveness, remain excluded from actual decision-making authority in the central task force. This combination preserves the legitimacy of the process while narrowing its transformative horizon while paying lip service to inclusivity. Financing without redistribution of power Availability of finance is one of the important compulsions behind the GHA reform agenda. According to the WHO Executive Board Document EB158/44 on GHA Reform: “The contraction of ODA in 2025 and strain on the multilateral system have aggravated weaknesses in GHA governance, coordination and financing, increasing fragmentation, service disruptions and risks to global health functions.” Further, it states: “Alongside the growing pressure on global health actors to refocus and rationalize resources, numerous initiatives, 7 papers and discussions on GHA reform have emerged, examining issues such as rationalizing the international financing of both global public health goods and development cooperation for health at the country level.” The financing pillar is especially revealing the proposal’s limited ambition. It commits to mapping existing flows and identifying options for improving support to national plans and budgets, but it does not commit to altering the underlying political economy of health financing. There is no meaningful proposal to expand assessed contributions at the scale required to loosen WHO’s dependence on earmarked voluntary funding, nor serious engagement with the debt constraints that limit fiscal space in many low-income and lower-middle-income countries. Pakistan, for example, warned against austerity-driven reform and stressed that “lean must not become synonymous with less…[A] genuine reform demands sustained and predictable financing, accelerated transfer of innovative technologies to build long-term self-sufficiency, while keeping national health system strengthening at its core.” The proposal is also silent on structural intellectual property reform and only weakly connected, if at all, to broader Global South efforts to reform international tax and financial governance. That silence matters. Financing alignment without fiscal redistribution leaves intact the asymmetries that produced the current crisis: countries are expected to assume greater ownership over health priorities while remaining constrained by debt burdens, intellectual property monopolies, volatile aid, and donor-shaped financing channels. Thus, the reform agenda remains concentrated on coordination, transparency, and efficiency rather than on reallocation of power or resources. In other words, it aims to leave sustainable finance availability to these entities causing fragmentation and reinforce a donor-fragmented system to work better, not to remake it on more democratic terms. Indeed, at the WHA79, the representative of Colombia questioned this agenda and asked directly: “What is being reformed, and why?”, warning that the process could have a “massive impact on WHO as a specialized UN agency.” Legitimization through WHO While Member States and civil society were responding to WHO surveys and participating in official briefings, the normative parameters of “global health architecture reform” were being shaped in a parallel circuit of high‑influence convenings: the One Health Summit in Lyon under the French G7 presidency, the Wellcome Global Convening, and the World Bank-IMF Spring Meetings, among others. These were not WHO‑convened processes, and access to them was heavily skewed toward institutionally resourced Northern governments, think tanks and philanthropic intermediaries. The Lyon Joint Political Declaration, adopted at the One Health Summit in April, is emblematic. Substantively, it endorses WHO‑hosted reform and echoes many Global South demands on sovereignty, equity and diversified financing. Politically, however, it derives its weight from being anchored in a G7 presidency, with heads of state, senior ministers and major funders in the room. That kind of declaration prejudges the WHO process: it sets expectations and defines the corridor of acceptable policy options. Formal multilateralism is thus placed in the position of legitimizing a narrative largely framed outside the WHO.
This dynamic is not unique to health; it is symptomatic of a wider crisis in global governance itself. The G7 summit in Évian, France in June 2026, where leaders and frontier technology firms debated wars, AI and global economic imbalances, offers a textbook example of small‑circle governance: a self-selected club of advanced economies plus invited partners debating global rules in a format that excludes majority of countries. In parallel UN-led negotiations on regulating military AI proceeded next door in Geneva with far less media attention and political weight. The architecture of influence is legible in the seating plan: the heads of international financial institutions and Big Tech sit at the centre of G7 discussions, while the UN system’s core normative bodies deliberate at the margins. What is at stake, in health and in AI governance alike, is not only which actors attend which discussion, but which processes get to define the agendas and policies. This is precisely the pattern that China’s “more just and equitable global governance” White Paper seeks to name and contest: an international order where small circles and exclusive blocs increasingly pre‑structure universal multilateralism, and where the Global South’s formal inclusion rarely translates into equivalent influence. WHA79 and the struggle over ownership Debates at WHA79 revealed that even the baseline principle that the process must be Member State-led had to be actively defended rather than simply assumed. During the meeting, Pakistan, Panama, Indonesia, Nepal, Mexico, China, Saudi Arabia and South Africa all stressed that ownership must remain with Member States and that Geneva-based consultations through Permanent Missions remain central. That this had to be said at all is politically revealing. In principle, a reform of a specialized UN agency should obviously be led by its Member States. In practice, however, contemporary global governance increasingly privileges “swift,” “efficient,” and “lean” processes in which political authority is displaced by seemingly technocratic management, donor influence, and multi-stakeholder informality. The fact that Global South countries had to fight to reaffirm a principle that ought to have been self-evident shows how far universal multilateral norms have eroded under the pressure of fragmented governance. Northern delegations tended to frame reform as a lean, cost‑neutral exercise, while Global South States argued that this risks entrenching austerity rather than enabling structural change. Global South interventions emphasized the need for sustained and predictable financing, technology transfer, and health system strengthening, and warned that the reforms could fundamentally alter WHO’s multilateral character if they are not explicitly protected from commercial capture. They highlighted risks of undue influence, linking the process to equity commitments in the Pandemic Agreement. The debate exposed a deeper contradiction. The formal language of inclusivity remains intact, but the actual terms of participation and authority are increasingly contested. Global South delegations were not merely discussing administrative design; they were defending the residual political authority of Member States within a governance environment that now routinely treats intergovernmental deliberation as an obstacle to speed and managerial efficiency. The GHA Reform Process Reflects the Politics The WHO GHA reform process, therefore, cannot be understood as a purely technocratic exercise. It is an arena where competing visions of multilateralism confront one another: one that privileges flexible, donor-steered networks of funds, partnerships, and clubs, and another that insists on stronger public, universal, and Member State-centered institutions. The interventions from Global South delegations at WHA79 were far from routine. They were explicit warnings against allowing GHA reform that manages, rather than rectify, a fragmented GHG order. The current GHA reform agenda carries the risk of formalizing the status quo by conferring legitimacy upon the very entities whose existence has fundamentally splintered global health governance, diverted resources, and privileged private and powerful interests. Whether the process ultimately produces meaningful structural change will depend on which coalition succeeds in shaping its practical assumptions over the coming year. The GHA reform process would largely be confined to efficiency gains, financing alignment, and improved coordination among already powerful actors; it will consolidate rather than transform the current governance. Hence, Member States (especially from the Global South) need to link the process to broader struggles over fiscal sovereignty, technology transfer, debt justice, and democratic multilateralism. The reform could become part of a larger effort to reclaim GHG from fragmented and donor-dominated control. (* Faculty Member, United Nations University Global Health)
|
||